Elog-general medicine
25th November 2020
55 yr old Male with
Pain with abdomen since 3 months
This is an online E log book to discuss our patient's
de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
CASE PRESENTATION:





This is a history of a 55 year old Male, farmer
by occupation came with chief complains of
C/o pain in abdomen since 3month
C/o distention abdomen since 3 months
C/o yellowish discoloration of urine and eyes since 2 months
C/o loss of appetite and c/o weakness
Patient was apparently asymptomatic 3 months back then developed pain in abdomen in Rt lumber and Rt hypochondrium which is insidious in onset, rapidly progressive in nature ,burning type of pain, radiating to epigastrium and retrosternal region aggravated on eating food and relieved on taking medication.
Pain was persistent through out the day relieved only on taking medication was on ''TRAMADOL INJ'' Since 3 months .
H/O icterus since 2 months,gradually progressive.
C/o vomiting 1 episode , 2 days back, non-bilious,no hematemesis.
C/o nausea
No h/o passing stools since 2 days ,passing flatus
No h/o bleeding per rectum
No h/o significant loss of weight
Loss of appetite present
No h/o fever associated with pain
No h/o high coloured urine/clay coloured stools
Not a known case of diabetes and hypertension.
No history of TB, epilepsy, thyroid and asthama.
No h/o previous surgeries.
Decrease appetite
Mixed diet
Sleep adequate
Irregular bowel and bladder movements
Not passing stools since 2 days
Smoker- tobacco (6 beedis) per day since 20 years.hm H/o kaini consumption
Alcoholic since 7 years
No known allergies.
General examination:-
Patient is conscious,coherent and cooperative
Thin built and poorly nourished


No pallor, clubbing, cyanosis, lymphedenopathy, edema
Icterus present since 2 months

Temperature-98.2F
Bp- 100/60mmhg
PR- 86bpm
RR- 32cpm
Sp02- 99%
GRBS - 126mg/dl
SYSTEMIC EXAMINATION:-
P/A :- shape- scaphoid,umbilicus - central, soft,tenderness in Rt hypochondrium and umbilical region. Non-distended. NO Organomegaly, tennis ball like mass palpable on deep inspiration.


CVS - S1S2 +,no murmurs
RS - BAE+,NVBS+
CNS - intact
Referred to surgery for pain in abdomen and mass in abdomen on rt hypochondrium and rt lumber region.
Advice:
1) inj.vit k 1 amp IM OD 3days
2) start antibiotics if patient develops any signs of cholangitis (fever,chills and rigors)
INVESTIGATIONS:-
LFT :-
TB- 10.38
DB- 6.01
AST - 86
ALT - 150
ALP - 909
TP - 6.1
Alb- 3.7
A/G ratio - 1.56
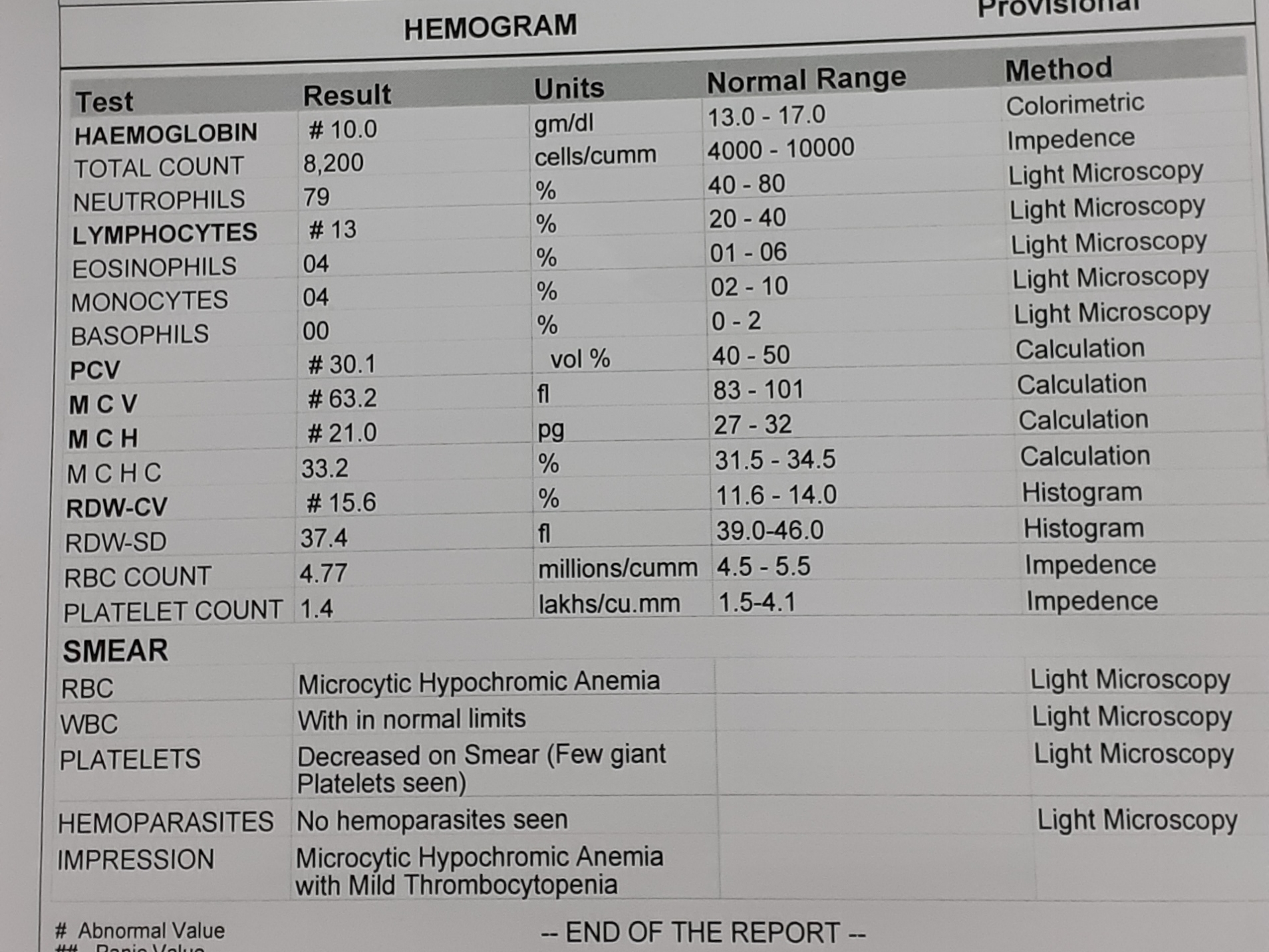
Hemogram:-
Hb - 10mg/dl
Tc - 8200 cells/cumm
PC - 1.4 lakhs/cumm
Serology- negative



Ultrasound abdomen:


Chest xray PA view:

Ecg:
4) inj.tramadol 1 amp in 100ml NS/IV/slow
Day1













Ultrasound Review:



















Referral to oncology




Reffered to gastroenterologist:

He presented with pain abdomen,icterus,loss of appetite with investigations done outside showing
Dilatation of cbd, multiple duodenal ulcers,
First endoscopy was done to look for obstruction in the second part of duodenum and growth beneath the ulcers, no such findings reported
Then mrcp was planned to look for area of obstruction,mainly the periampullary area, findings suggested a narrowing of cbd duct at it's terminal part and abnormal dilatation,
Surgical oncologist was consulted , and triple phase ct was adviced to see the presence of lymphadenopathy, and extent of local invasion for ? cholangiocarcinoma which was our working diagnosis
CT revealed a stricture at the terminal part of cbd with no evidence of growth , lymphadenopathy, which led us to our current differentials of
? primary sclerosing cholangitis
? cholagiocarcinoma
IgG4 related disease.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5953192/Treatment of IgG4 Related disease
DIAGNOSIS:
Obstructive jaundice 2° to CBD stricture
2° to IgG4 Related disease
? primary sclerosing cholangitis
TREATMENT:-
In a retrospective, multicenter study of 25 IgG4-RD patients in France, prednisone at a starting dose of approximately 47 mg/day (0.67 mg/kg for a 70-kg patient) was effective in controlling the disease in 90% of patients. In that study, treatment response was defined by the presence of at least two of the following features: improved clinical status, reduction in serum IgG4 concentration, and improved radiologic findings. Even higher response rates have been reported in autoimmune
Day1
1) T.ultracet PO QID
2)T.Prababilin 75mg PO/OD
3) T.Amitriptylline 10mg PO/HS
5) Inj.Voveran 2cc IM sos
Day2,3
1) T.ultracet PO QID
2)T.Pragabalin 75mg PO/OD
3) T.Amitriptylline 10mg PO/HS
4) inj.tramadol 1 amp in 100ml NS/IV/slow
5) Inj.Voveran 2cc IM/sos
6)Mucaine gel 15ml PO/TID/15mins after food
7) Inj .Pantop 40mg IV/BD
Day 4
1) T.ultracet PO QID
2)T.Pragabalin 75mg PO/OD
3)T. Amitriptylline 10mg PO/HS
4) inj.tramadol 1 amp in 100ml NS/IV/slow
5) Inj.Voveran 2cc IM/sos
6)Mucaine gel 15ml PO/TID/15mins after food
7) Inj .Pantop 40mg IV/BD
8) I/O charting
9)temperature, BP, PR 4th hourly monitoring
10)GRBS 6th hourly monitoring
Day 5
1) T.ultracet PO QID
2)T.Pragabailin 75mg PO/OD
3) T.Amitriptylline 10mg PO/HS
4) inj.tramadol 1 amp in 100ml NS/IV/slow
5) Inj.Voveran 2cc IM/sos
6)Mucaine gel 15ml PO/TID/15mins after food
7) Inj .Pantop 40mg IV/BD
8) I/O charting
9)temperature, BP, PR 4th hourly monitoring
10)GRBS 6th hourly monitoring
Day 6,7,8
1) T.ultracet PO QID
2)T.Pragabailin 75mg PO/OD
3) T.Amitriptylline 10mg PO/HS
4) inj.tramadol 1 amp in 100ml NS/IV/slow
5) Inj.Voveran 2cc IM/sos
6)Mucaine gel 15ml PO/TID/15mins after food
7) Inj .Pantop 40mg IV/BD
8) I/O charting
9)temperature, BP, PR 4th hourly monitoring
10)GRBS 6th hourly monitoring
Day 9
1) T.ultracet PO QID
2)T.Pragabailin 150mg PO/OD
3) T.Amitriptylline 10mg PO/HS
4) inj.tramadol 1 amp in 100ml NS/IV/slow
5) Inj.buscopan 2cc IM sos
6)Mucaine gel 15ml PO/TID/15mins after food
7) Inj .Pantop 40mg IV/BD
8) I/O charting
9)temperature, BP, PR 8th hourly monitoring
10)GRBS 12th hourly monitoring
Day 10,11,12
1) T.ultracet PO QID
2)T.Pragabailin 150mg PO/OD
3) T.Amitriptylline 20mg PO/HS
4) inj.tramadol 1 amp in 100ml NS/IV/slow
5) Inj.buscopan 2cc IM/sos
6)Mucaine gel 15ml PO/TID/15mins after food
7) Inj .Pantop 40mg IV/BD
8) I/O charting
9)temperature, BP, PR 12th hourly monitoring
10)GRBS 12th hourly monitoring
Day 14
1) T.ultracet PO QID
2)T.Pragabailin 75mg PO/OD
3) T.Amitriptylline 10mg PO/HS
4) inj.tramadol 1 amp in 100ml NS/IV/slow
5) Inj.buscopan 2cc IM/sos
6)Mucaine gel 15ml PO/TID/15mins after food
7) Inj .Pantop 40mg IV/BD
8) T.Prednicolone 40mg PO/OD-day 1
9)temperature, BP, PR 12th hourly monitoring
10)GRBS 12th hourly monitoring
Day 15-24
1) T.ultracet PO QID
2)T.Pragabailin 150mg PO/OD
3) T.Amitriptylline 20mg PO/HS
4) inj.tramadol 1 amp in 100ml NS/IV/slow
5) Inj.buscopan 2cc IM/sos
6)Mucaine gel 15ml PO/TID/15mins after food
7) Inj .Pantop 40mg IV/BD
8) T.Prednisolone 40mg D2-11
9) T.Nicotex gums 2mg sos( whenever pt experiences craving for tobacco
10)temperature, BP, PR,GRBS 12th hourly monitoring


{kind=link}
Really awesome blog. Your blog is really useful for me. Thanks for sharing this informative blog. Keep update your blog.
ReplyDeleteGeneral Medicine